


More than a message: Framing public health advocacy to change corporate practices
Wednesday, June 01, 2005If they can get you asking the wrong questions, they don't have to worry about the answers. — Thomas Pynchon (2000)
Public health educators are often confronted by challenging arguments from companies that produce harmful products. Tobacco companies say they sell a legal product. Alcohol companies insist that most people drink responsibly and that the companies should not be blamed if some people abuse their products. Junk food purveyors say that it is the parents' responsibility to control what children eat. Car companies say that the key to greater safety on the road is changes in drivers' behavior.
Public health educators often struggle to respond to such arguments. They are put on the defensive, and the language does not come easily. It is no wonder — after all, each industry argument is truthful, if incomplete. One reason public health advocates have difficulty responding may be that they do not understand that public health language needs to be rooted in a framework of values. The good news is that in fact, public health has a clear, consistent set of values that can guide health educators' messages. Just as the corporate arguments are organized along a consistent set of values, public health advocates can reframe issues with the same level of confidence and consistency to reflect broader public health goals.
Public health and social justice
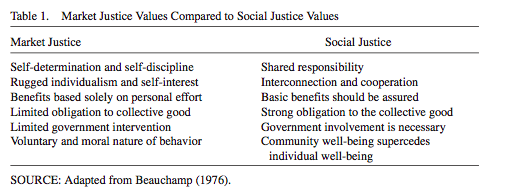
For more than a generation, public health practitioners have been guided by the work of Daniel Beauchamp (1976), who argues that the ethic of public health is social justice. "Public health should be a way of doing justice," Beauchamp wrote, "a way of asserting the value and priority of all human life" (p. 8). Beauchamp called for newly constructed collective definitions of public health problems that clearly communicate "that the origins of [death and disability] lie beyond merely individual factors" (p. 9), despite the fact that individual factors must, of course, be acknowledged.
The biggest barrier to achieving social justice is the competing ethic of market justice. Market justice is rooted in the basic notion of Adam Smith's (2000) invisible hand, the idea that the market will naturally respond to the desires of the people and so the unfettered marketplace is the best way to serve those desires. Market justice ideals have long dominated political and cultural life in the United States. Much of the debate on policy issues concerns whether or how to restrain the marketplace with regulation. Regulation is always seen as a constraint on the free market, to be tolerated only in limited circumstances.
It is no surprise then that market justice dominates current thinking and practice in public health. Politicians' focus on tax cuts as a means of unleashing market power and solving societal problems is a good example of how public health suffers when market justice predominates. Services for helping people and policies for protecting people are left unfunded as tax cuts are embraced and available funds disappear. Without a shift to social justice, says Beauchamp (1976), progress in public health will be thwarted. A shift to stronger social justice values would bring greater public health gains for communities and individuals because policies to ensure equitable public health outcomes would be put in place to counter the ill effects of the market (see Table 1).
{kind=link}
The fight against tobacco can be seen as one clearly successful example of the shift that Beauchamp (1976) advocated. Tobacco has been fundamentally redefined from an individual problem called smoking to a public issue called tobacco, from a focus on blaming the smoker to a focus on the role of industry and the government. Consequently, strategies are now directed toward creating rules that hold the tobacco industry disproportionately, but fairly, accountable for the death and disability it has caused. A new definition of the problem exposed the limits of the norm of individual responsibility, challenged the market justice ethic driving public policy, and made room for a shift toward collective solutions emphasizing social justice. Public health is, arguably, a long way from completing its task, but surely, the tide has turned and we are headed toward a world with less tobacco, not more.
Practitioners working in other public health arenas are now eyeing tobacco control enviously, wondering if similar tactics will work to advance fairer policy approaches to obesity and other public health problems. Certainly, this is possible and there is much to learn from successes, and failures, in tobacco control. Fundamentally, however, the shift must be tied to a core set of values, and for public health, those values should reflect social justice. As Beauchamp (1976) explains,
The central problems remain the injustice of a market ethic that unfairly protects majorities and powerful interests from their fair share of the burdens of prevention, and of convincing the public that the task of protecting the public's health lies categorically beyond the norms of market-justice. This means that the function of each different redefinition of a specific problem must be to raise the common and recurrent issue of justice by exposing the aggressive and powerful structures implicated in all instances of preventable death and disability, and further to point to the necessity for collective measures to confront and resist these structures. (p. 10)
The aggressive and powerful structures implicated in market justice forces can often be traced to corporate actors. This understanding does not negate the value of individual liberty in our society, but it does suggest that those values must be balanced with other values that emphasize the common good, including health. Public health advocates often argue that individual freedom is taken to the extreme when companies are permitted to profit regardless of the consequences for health and safety, whereas industries insist that they have the right to promote products that are legal. How public advocates make the case for their position will influence which ethic comes to dominate public health policy, because how they argue for change, including the language they use, can either reinforce social justice values or undermine them.
The language of public health
The dominant language, what sociologists Bellah, Madsen, Sullivan, Swidler, and Tiptom (1985) called the first language, of America is individualism and personal responsibility. The central idea is that rugged individualism, self-discipline, and selfdetermination are the key variables for success in American society. Indeed, a Pew Center Poll (2002) conducted in 44 countries found that people in the United States were much more likely to believe that they are in control of their lives than to see their lives as subject to the effect of external forces. Thus, self-determination, personal discipline, and hard work are seen as dominant factors, reinforcing individualism. A shift to social justice demands a rebalancing of these values with others that Americans also hold (Wallack & Lawrence, in press).
It is in this redefinition that language comes into play. Recent explorations by political scientists (Harrington, 1999; Reich, 1990; Tronto, 1994), sociologists (Gamson, 1992), and cognitive linguists (Lakoff, 1996) offer new tools to public health educators who want to communicate stronger social justice values.
Language is important to public health practitioners because how an issue is described, or framed, can determine the extent to which it has popular or political support. Language communicates thoughts and ideas, and certain words and phrases shape the way people think about issues. Framing battles in public health illustrates the tension in our society between individual freedom and collective responsibility, which Beauchamp (1976) articulated in terms of market justice and social justice. Recent analyses of language from various fields explain how frames influence public dialogue on social issues, with important consequences for public health. Using these new rubrics, we compare and contrast arguments used to oppose or support public health goals. We then identify the common public health frames across these issues to illustrate how clear, concise language, anchored in social justice values, can effectively reframe issues, concluding with lessons for health educators who need to frame public health issues effectively. Our focus is on debates involving corporate practices that harm health, but the principles apply in other contentious and controversial policy contexts.
A caveat: Language is never first of foremost
Although language is a crucial expression of public health values, it should never be an advocate's first and foremost consideration. Before determining what to say, public health advocates must determine what they want to change in concrete terms, the more specific, the better (Chapman, 2001; Themba, 1999). And advocates need to know how to create the change (Chapman & Lupton, 1994; Wallack, Dorfman, Jernigan, & Themba, 1993; Wallack, Woodruff, Dorfman, & Diaz, 1999). Only then should they turn to considerations of language. The language public health educators use needs to grow out of policy that needs first to be rooted in social justice values.
Still, close attention to language is necessary and important because it is how public health advocates make their case for the change they want and a key mechanism with which they communicate their values. Once the steps to a solution for a given public health problem have been identified and the mechanisms for instituting them have been determined, then language should be developed to communicate the solution and why it matters. That language, the specifics of the message, will then emerge from how the issue is being framed.
Framing: What it is, why it matters
Framing means many different things to people. Some think of framing as finding the right word, whereas others believe that frames tap complex moral structures that trigger how people react to a whole constellation of social and public policy issues in our society. We describe two types of frames — conceptual frames and news frames — that we believe have the most bearing on how to create messages that emphasize public health as social justice.
Conceptual frames
Lakoff (1996), a cognitive linguist, argues that frames are the conceptual bedrock for understanding anything. People are only able to interpret words, images, actions, or text of any kind because their brains fit those texts into an existing conceptual system that gives them order and meaning. Just a few cues, a word or an image, trigger whole frames that inspire certain interpretations in audiences. Frames are often expressed in metaphors that people routinely use to understand abstract issues: "Horse race metaphors are common in political campaigns; war metaphors are common in discussion of health threats; and sports and business metaphors are common in other areas" (Lakoff & Morgan, 2001). For example, the California Chamber of Commerce regularly issues a list of job-killer legislation it tries to defeat. The term is simple and evocative. Killer implies that someone is coming after you and that the situation is threatening, even dire. Killers must be stopped. They must be punished. Their targets need immediate protection and defensive maneuvers. The frame evokes these ideas before we have even an inkling of what the specific legislation might be about. In fact, if the chamber is successful with its job-killer frame, it will not ever have to debate the merits of the bill. The frame will preempt any discussion about the benefits of the legislation.
Political scientist Gilliam (2003) explains that frames are the "labels the mind uses to find what it knows." Frames are a composition of elements — visuals, values, stereotypes, messengers — which together trigger an existing idea. They tell us what this communication is about. They signal what to pay attention to (and what not to), they allow us to fill in or infer missing information, and they set up a pattern of reasoning that influences decision outcomes. Framing, therefore, is a translation process between incoming information and the pictures in our heads (Gilliam, 2003).
It takes very few words to trigger a frame. Consider this example from a poll The New York Times conducted in 2000. By changing just a few words, pollsters registered a marked difference in audience response. When asked whether leaders in Washington should allocate an expected budget surplus to tax cuts or government programs, 60% chose tax cuts. But when asked the same question in a slightly different way, "should the money be used for a tax cut, or should it be spent on programs for education, the environment, health care, crime-fighting, and military defense" (i.e., government programs), 69% chose the more tangible list. Small differences in the poll question elicited significantly different responses, illustrating the power of language. But more than just the word, it is the conceptual framework that the word government evokes that is critical here. Government, in this instance, triggers interpretations such as waste, inefficiency, or giving people something for nothing, all of which undermine the role of public health.
Framing levels move from values to strategy
Lakoff describes three conceptual levels for framing messages in the context of public health and other social or political issues (G. Lakoff & P. Morgan, personal communication, June 1-30, 2004). Level 1 is the expression of overarching values, such as fairness, responsibility, equality, equity, and so forth, the core values that motivate us to change the world or not change it. Level 2 is the general issue being addressed, such as housing, the environment, schools, or health. Level 3 is about the nitty gritty of those issues, including the policy detail or strategy and tactics for achieving change.
Messages can be generated from any level, but Level 1 is most important because it is at Level 1 that people connect in the deepest way. According to Lakoff (1996), people's support or rejection of an issue will be largely determined by whether they can identify and connect with the Level 1 value. Values are motivators and messages for social change should reinforce and activate values. Messages, therefore, should articulate Level 1 values and not get mired in Level 3 minutiae. Public health advocates must know the Level 3 details (e.g., what needs changing and how the change will occur), but those details need not be prominent in the message. In fact, if Level 3 details crowd out Level 1 values, Lakoff contends that the message will be less effective.
The difference between how Level 1 and Level 3 are expressed in messages is nicely illustrated in an example from how health care was discussed in the 2004 presidential campaign. Quotes from President George W. Bush and his Democratic challenger, Senator John Kerry, are easily recognizable as Level 1 and Level 3 messages. In a radio story early in the campaign, National Public Radio reporter Julie Rovner compares the health plans being touted by Bush and Kerry, noting the details and differences between them, including the fact that Kerry's plan will cover a far greater percentage of the uninsured than Bush's plan would. At different points in the story, she includes a statement, passionately delivered, from each man:
President Bush: The debate is about whether or not the marketplace ought to have a function in determining the cost of health care or whether or not the federal government should make all decisions. I've made my stand. I believe that the best health care policy is one that trusts and empowers consumers, and one that understands the market. Senator Kerry: Have your co-pays gone up? Have your deductibles gone up? Then you need to tell this administration that we're fed up, and their time is up ... [my plan] will reduce the average premium by $1,000 a year and it will crack down on the skyrocketing drug prices we face today. (National Public Radio, 2004)
Rovner notes that President Bush's concern is less about the differences between the plans and more about values. Indeed, President Bush's statement about health care clearly reflects his Level 1 market justice values, whereas Senator Kerry's statement focuses on the details of the plan, a Level 3 frame. If the market justice perspective around reforming health care dominates debate at Level 1, reinforcing the idea that the market will solve the problem with minimal government action, it does not matter how forcefully advocates can argue the details of the policy at Level 3. This is because, as Lakoff (1996) says, frames trump facts, and the frame is set at Level 1. To compete with Bush's statement and reframe the debate, Kerry would have to make a similarly strong statement communicating his Level 1 values, perhaps based on what he believes is fair and right for Americans rather than the details of how the plan will operate.
Of course, simply because the Level 1 frame is asserted does not mean it will carry the day; there are many factors at play that influence the outcomes of elections and policy debate, and framing is only one, however important. It is also worth noting that unfortunately, advocates' tendency is to argue the fallacy of their opponent's Level 1 frame, in this case, the basic idea that an unfettered marketplace will solve the health care crisis. Cognitive linguists and other communications scholars suggest that advocates should resist this impulse because such arguments will only reinforce the existing frame. Thus, public health advocates will have the strategic advantage when they set the Level 1 frame themselves, not when they respond to an opponent's frame that has already been set.
The theoretical and empirical work on Level 1 values and how they affect messages is nascent but likely to be important and valuable to public health educators because, in general, many are more adept at describing Level 3 details than they are at integrating Level 1 values. Insofar as Level 1 values set the frame, the advantage will be with those groups who most easily and frequently trigger their values in key audiences.
Different Level 2 issues can share the same Level 1 values. Below are sample messages from three different issues — tobacco, alcohol, and affordable housing — that share the same Level 1 value, in this case fairness and equity. The policies used here are examples, and at any given time, the specifics of the policy may change. When they do, the values statement may remain consistent, or it too may change.
For alcohol, with a Level 3 policy goal of limiting the number of places alcohol is sold, the message might be the following:
Too many liquor stores detract from the quality of life. It is not fair that certain families are subjected to such degraded conditions. Every family should have the opportunity to raise their children in a healthy environment. The city should make a rule to limit the number of liquor stores allowed within a certain radius.
For tobacco, with a Level 3 policy goal of enacting clean indoor air laws across all sectors of the city, the message might be the following:
While we have achieved great progress in reducing smoking, there are still large populations, primarily in low income communities of color, that are regularly exposed to toxic secondhand smoke. It is not fair that some of our cities' workers are protected and others are not. We should enact uniform clean indoor ordinances to protect workers in all workplaces, including restaurants and bars.
For affordable housing, with a Level 3 policy goal of providing rent subsidies to low income families, the message might be the following:
People who need housing can't get it even though they work two jobs. Without a place to live, basic family life is shattered. It is not fair that hard-working people cannot find an affordable home. The city council should pass the rent subsidy resolution immediately.
News frames
Conceptual frames operate inside our heads to organize and interpret the cues we get from the world. But where do the cues come from? In greater numbers than ever before, people in our society get their information, especially what they know about any person or situation they don't personally experience, from the media, especially the news. Although the entertainment media transmit ideas and mores through popular culture, the news is the site for our public conversation, the place where policy issues are debated and framed. As early as 1922, commentator Walter Lippmann warned that news was functioning to provide the pictures in our heads that were determining policy decisions. The news, then, is an important source of frames as well as the terrain on which public health policy is debated and so warrants a closer look. What we find is that the routines of producing news have shaped typical news frames in ways that make public health stories that communicate social justice values harder to tell.
In the context of news, frames organize the meaning in stories, delineating what is and is not important. Communications researcher Robert Entman (1993) suggests four functions of news frames:
Frames ... define problems — determine what a causal agenda is doing with what costs and benefits, usually measured in terms of common cultural values; diagnose causes — identify the forces creating the problem; make moral judgments — evaluate causal agendas and their effects; and suggest remedies — offer and justify treatments for the problems and predict their likely effects. (p. 52)
Similar to a frame around a painting, the news frame draws attention to a specific picture and separates told from untold pieces of the story. Elements in the story are said to be in the frame; elements left out of the story are outside the frame and are thought to be unimportant or less legitimate.
News frames can also refer to the structure of a story. Sociologist Todd Gitlin (1980) notes that frames are "persistent patterns" by which the news media organize and present the news so that it concerns "the event, not the underlying condition; the person, not the group; conflict, not consensus; the fact that 'advances the story,' not the one that explains it" (p. 28). The structural pattern is evident in newspaper stories but is even more pronounced in local and network television news.
Political scientist and communications scholar Shanto Iyengar (1991) demonstrates that (a) most television news is framed in terms of individuals and events, what he called "episodic," and (b) audiences interpret episodic stories in ways that tend to blame the victim.
According to Iyengar (1991), when people watch news stories that lack context, they focus on the individuals. Without any other information to go on, viewers tend to attribute responsibility to the people portrayed in the story for the problem and its solution. In other words, they blame the victim. Without a sense of the forces that brought the people in the story to this point, viewers are likely to distance themselves from the "victims" portrayed, assume that those portrayed in the story brought it on themselves, look to them to work harder to solve their own problem or accept the consequences of their behavior. Watching episodic stories, viewers gain no insight into the larger social and political circumstances that contribute to the individual problem.
It is not surprising that the most prevalent news frames would inspire interpretations of personal responsibility in audiences. As an integral part of American culture, the media reflect the dominant values of that culture. So the first language of America, individualism, is also dominant in news portrayals.
To counter this dominant news frame, advocates must help reporters do a better job describing the landscape surrounding individuals and events so the context of public health problems becomes visible. Iyengar (1991) called these stories thematic.
Thematic stories may engage viewers with a personal story, but they also give them more: background, consequences, and other information that provides context. Iyengar (1991) found that viewers who see thematic stories understand that responsibility is shared between individuals and their institutions and found that viewers are more likely to recognize that the government or other institutions have a role in solving the problem.
Typical news frames are more often portraits than landscapes
A simple way to distinguish story types is to think of the difference between a portrait and a landscape (Dorfman, 2003). In a news story framed as a portrait, audiences may learn a great deal about an individual or an event, with great drama and emotion. But it is hard to see what surrounds that individual or what brought him or her to that moment in time. A landscape story pulls back the lens to take a broader view. It may include people and events, but it connects them to the larger social and economic forces. News stories framed in such a manner are more likely to evoke solutions that do not focus exclusively on individuals but also on the policies, institutions, and conditions that surround and affect them.
The key value that is affected by portrait and landscape frames is responsibility. News stories focused on people or events evoke feelings of personal responsibility in audiences. Landscape stories evoke shared responsibility between individuals and institutions. Advocates should strive to make stories about the landscape as vivid and interesting as the portrait. This is not easy to do but is crucial. The framing challenge for public health educators is to create landscape stories that are as compelling as portraits and include Level 1 values statements.
There are economic imperatives in the media business that compel reporters to pursue portraits rather than landscapes. Corporate concentration has forced news outlets to abandon public interest goals to pursue profit in the form of larger audiences (Bagdikian, 2004). Stories framed as portraits serve that purpose better than landscapes because they are easier stories to tell and presumably attract a larger audience.
Framing public health
Public health issues, such as tobacco, alcohol, guns, and traffic safety, have all experienced a transition from a focus on behavior to attention to policy that affects the environments in which the behavior takes place. The issue of drinking and driving provides one example. In the 1950s, the issue was barely visible as a public health problem. Drivers had "one for the road" before they left the bar. Alcohol problems were personal problems and the remedy was to drive defensively. The development of a national focus on alcohol problems coalesced in the 1970s with the formation of the National Institute on Alcohol Abuse and Alcoholism, which began concentrated government support for research and intervention. The issue gained greater visibility in 1980 when Mothers Against Drunk Driving (MADD) was founded to support families of victims and advocate for cultural change regarding how society tolerated drunk drivers. Combining forces with public health advocates who investigated and promoted a variety of prevention strategies, MADD expanded its purpose and scope to focus on state policies across the country. The alcohol issue has matured during the past 50 years. Most states now have a .08 blood alcohol limit, and as a nation, we have a 21-year-old drinking age. Although many programs still focus on personal drinking behavior, others include such policy goals as reducing alcohol outlet concentration in the inner city, removing alcohol advertising that reaches kids, and raising excise taxes (Dorfman, Ervice, & Woodruff, 2002).
In fact, many health and social problems are related to conditions outside the immediate individual's control. A focus limited to personal behavior change ultimately fails us as a society because it narrows the possible solutions inappropriately. For example, individual children and their parents need to make healthy personal choices so they will grow up with strong bodies and sound minds. If they do that, we should have a healthier society. But the choices are difficult and sometimes impossible. How can children get adequate exercise — important for establishing good habits and preventing childhood obesity and adult cancer — if there are no safe places to play? Or if physical education is no longer an available part of the school curriculum? Or if there are insufficient resources for after-school sports? Personal choices are always made in the context of a larger environment. Prevention can address both ends of the spectrum.
The language problem that ensues for public health educators derives from the challenges inherent in advocating for prevention that requires social or environmental change. Inevitably, environmental changes are more controversial than changes in personal behavior because they generally require a shift in resources or responsibility. The changes tap into Level 1 values, such as fairness and responsibility, and how those values are interpreted. For example, is fairness about being able to choose any vehicle one wants, no matter how unsafe or gas guzzling? Or is fairness about the government providing standards for products that protect health and safety? How should responsibility for auto safety be shared? These arguments will be contested in highly visible public settings, such as legislative hearings. (Personal behavior changes may also be contested but usually by individuals in private settings.) Typically, the debates surrounding the social changes, be they policies to restrict tobacco use, limit access to alcohol, change the way motor vehicles are manufactured, or ban certain firearms, will be carried out in the news.
Public health issues in the news
Research across various public issues has upheld Iyengar's (1991) findings that typical news stories are episodic, focused on individuals or events. Studies of childhood lead poisoning (Bellows, 1998), childhood nutrition policy (Woodruff, Dorfman, Berends, & Agron, 2003), immunizations and other children's health issues (Lawrence, 2002), injury and violence (Chavez & Dorfman, 1996; Dorfman & Schiraldi, 2001; Dorfman, Woodruff, Chavez, & Wallack, 1997; Jernigan & Dorfman, 1996; McManus & Dorfman, 2005), including the policy discussions surrounding guns (Woodruff & Villamin, 1997) and alcohol (Dorfman & Wallack, 1998), have found an emphasis on episodic stories, paralleling what Iyengar found on a variety of other issues in the news. Public health perspectives, in particular, are rare in news coverage. In one of the largest studies of local television news —more than 200 hours of local news broadcast across California in English and Spanish — only one story among 8,021 aired during a 12-day period, or about 2 minutes of news, was devoted to violence as a public health issue (Dorfman et al., 1997).
Studies of children's issues in the news have found an abundance of news that mentions children's health but, similar to the violence coverage, a dearth of in-depth reporting on the consequences of ill health or poor conditions for children, their families, or society at large. One study of childhood nutrition policy, for example, designed to maximize the number of policy-related stories, found that advice to parents was the single largest subject in the sample. The study found advocates describing the problem of childhood obesity using environmental, upstream concepts (e.g., "super-sizing," too much TV and sedentary activity, and fast food in schools), but when it came to describing solutions, they reverted to the individual and described personal behavior, generating individually oriented "news-you-can-use pieces," which reporters prefer but which may undermine a public health approach to childhood obesity (Woodruff et al., 2003). A follow-up study added childhood immunization, childhood injury, and children's health insurance to the mix and confirmed the earlier findings, going further to establish that although children's health policy is present in news stories, the values underlying the policies are rarely expressed (Lawrence, 2002).
Overall, the findings from the various studies suggest that public health issues are rarely portrayed in the news in ways that encourage audiences to comprehend and ponderthe underlying causes of problems or their potential policy solutions. Health stories, similar to other news, reinforce values of individualism and personal responsibility that feed the market justice perspective. This perspective comes out clearly in the comments from industry spokespeople in news stories and constitutes one of the more difficult challenges that public health educators must address, or reframe, in their own messages.
Anticipating the opposition frames
Because corporations' goal, and fiduciary responsibility, is to sell more of their products, their statements reflect a market justice value system. As former U.S. Surgeon General Antonia Novello (1992) noted, "one of the fundamental paradoxes of marketoriented societies is that some entrepreneurs — even acting completely within the prescribed rules of business practice — will come into conflict with public health goals" (p. 961). Corporate actors use all the resources at their command, including vast advertising and public relations budgets, to actively promote their market justice values.
The statements corporate spokespeople make in the face of public health challenges are remarkably similar. Statements from various industry spokespeople opposing public health measures generally reflect Level 1 market justice values: first, what's needed is more personal responsibility, not government regulation; second, as a precursor to taking personal initiative, education can solve the problem; and third, if the issue involves children or youth, this is really the parent's responsibility (see Table 2).
{kind=link}
Public health advocates can use the insights from the framing literature to anticipate and counter these frames by constructing messages that incorporate their own Level 1 values into concise descriptions of the problem and what should be done to address it.
The components of a message
Advocates can influence interpretations in any context by triggering frames that connect to their values. They can influence interpretation of news stories by creating news that makes the context visible. Effective messages meld specific policy demands with value statements that are delivered by strategically chosen messengers to specific targets. They are framed to emphasize Level 1 values and illustrate the landscape. Advocates can structure their messages this way by clearly and simply specifying the components of a message using three questions: (1) What's wrong? (2) Why does it matter? (3) What should be done about it?
The first question forces advocates to make a clear statement of concern. It flows directly from the overall strategy, which advocates should determine before they construct their message. Too often, advocates try to tell journalists everything they know about the issue, because they feel this may be their only opportunity to convey the enormity and importance of the problem. They should resist that urge. It is impossible to be comprehensive and strategic at the same time. Instead, public health advocates should focus narrowly on just one aspect of the problem and be able to describe it succinctly. Once that portion of the problem is being addressed, they will be able to shift their policy goal and message to focus on another aspect of the problem.
The second question represents the value dimension. This is the place for advocates to shout their Level 1 value, to say what is at stake. Several studies show that advocates do not do this enough. In news coverage, the value component is often absent (Chavez & Dorfman, 1996; Dorfman & Schiraldi, 2001; Dorfman & Wallack, 1998; Dorfman et al., 1997; Jernigan & Dorfman, 1996; Lawrence, 2002; McManus & Dorfman, 2005; Woodruff et al., 2003; Woodruff & Villamin, 1997). Values should be specific, clear, and describe why the target audience (often a single policy maker) should care. Advocates can use this part of the message to call on their target's sense of fairness, duty, or fiscal responsibility.
The third question articulates the policy objective. A common pitfall is that advocates expend so much energy communicating about the problem that when the inevitable question about the solution is asked, they are ill prepared to answer it. They give vague responses such as "well, it is a very complex problem with many facets, so the solution is complicated" or "the community needs to all come together." Certainly these responses are truthful, but they are not strategic; they do not advance the issue toward a specific solution. More effective by far is to answer with a specific, feasible solution, even if it is an incremental step toward the larger goal. This is not to say that there is only one solution to complex and difficult public health problems but rather that solutions generally evolve from small steps over time.
As an example, consider this core message used to publicize a study of fast food sold in California high school cafeterias, released by California Project Leaders Encouraging Activity and Nutrition (LEAN; a project of the California Department of Health Services) and the Public Health Institute in 2000. The study highlighted the surprisingly high percentage of high schools with branded fast food outlets on campus and called for institutional solutions at both the local school district and state government levels. The core message, in terms of the three questions above, was as follows:
a. What's wrong? Fast food is widespread on high school campuses.
b. Why does it matter? Fast food on campus contributes to youth obesity and endangers the health of the next generation.
1. What should be done? Two solutions are key: (a) Schools must promote appealing, affordable healthy food options for students, and (b) the government must provide adequate funds for food service (so that local school districts do not have to supplement their budgets by contracting with fast food vendors).
Project LEAN's message reflects a strategic approach to communicating about obesity prevention. The problem statement does not attempt to describe every facet of life that may contribute to youth obesity; it focuses on the specific problem of fast food sold on high school campuses. The values statement, although it could be more explicit, calls for responsible action to protect the health of the next generation. The solution statement articulates two concrete policy actions that, although not intended to solve the entire problem of obesity, will certainly make a difference in the environment within which schools and students are making their nutrition-related decisions.
The benefit of developing and adhering to such a focused and strategic message statement was apparent in the news coverage that followed the release of the 2000 California High School Fast Food Survey. The event resulted in substantive news articles and opinion pieces in many California newspapers, many of which reflected the frame of shared institutional responsibility for addressing the problem of youth obesity. By contrast, many of the other news pieces on nutrition issues appearing during the same period were more likely to be superficial food features that resorted to traditional, individual-oriented advice about diet and exercise habits (Woodruff et al., 2003).
A news story that features an important public health issue can do more harm than good if it reinforces a blaming-the-victim frame for the cause and treatment of the problem and excludes the role for government and other institutions in solving the problem. This means that public health advocates must (a) be aware of the limited reach of most news frames and (b) work harder to help reporters focus more broadly, including on the social conditions and historical context beyond the individual or event, if they want key audiences to understand that responsibility for solutions to health problems must be shared across individuals and institutions, including the government. Left to their own devices, reporters will opt for the simple but interesting story about individual triumph or tribulation. But as Iyengar (1991) reminds us, "by simplifying complex issues to the level of anecdotal evidence, television news leads viewers to issue-specific attributions of responsibility, and these attributions tend to shield society and government from responsibility" (pp. 136-137).
Lessons for public health educators
Framing involves more than a message; knowing what change will advance public health interests comes first, followed by a clear analysis of what it will take to make the change happen. Once those fundamentals have been established, the next step will be developing a message strategy to make the case for the change because, if the change is significant, it will be contested. How the message is framed can either establish or bolster support for the change or reinforce the opposition. Public health educators can draw on three key lessons gleaned from the literature on framing and the news to increase their chances of making a winning case for social change:
a. understand and be able to articulate the core values and beliefs motivating the desired change;
b. articulate the components of messages so they integrate those values with a concise description of a key aspect of the problem and its corresponding, immediate solution; and
1. develop media skills to be able to deliver the message and compete effectively with adversaries, including the ability to make the landscape, or context, of the problem and solution visible to reporters.
The concepts underlying these lessons are being put to the test in defense of public health policies across issues and communities. Tobacco control advocates have perhaps the most collective experience and willingness to confront a market justice perspective. By now, their arguments are familiar and comfortable as they have spent decades challenging the idea that tobacco is simply a matter of personal choice. Although the tobacco industry remains a formidable opponent to public health interests and the fight is not over for the leading cause of preventable death, in that realm more than any other, advocates confidently reframe market justice values. Public health advocates working to reduce the harm from alcohol, guns, motor vehicles, lead, fast food, and a myriad of other issues will accelerate their progress as they strengthen their social change strategies and how they make the case for them.
By adopting these lessons, health educators will not create perfect messages that will stop the opposition in its tracks. Instead, better equipped to target their solutions and frame their messages, public health advocates will have renewed vigor for answering the frequent and forceful challenges they will receive any time they want to confront market justice norms and advance social justice values.
Conclusion
Many public health advocates share a fundamental worldview that reflects their values. They might not always agree on every issue or strategy, but they agree that the population's health is dependent not only on the choices individuals make but also the environments in which they make those choices. They recognize the interconnection between individual actions and the settings and circumstances surrounding those actions. They acknowledge that policy is an important tool for creating healthy environments.
Those who oppose public health policies see the world differently. The primary reason for society's progress, they believe, is personal initiative. Consequently, anything that inhibits that initiative is bad, and anything that fosters it is good. Public health advocates certainly do not eschew personal initiative, but they understand that it is constrained, or bolstered, by the world around it.
The discussion of values we have presented here may seem foreign to some in the field, particularly because another widely shared value in public health is objective science. Public health educators rightly search for evidence-based strategies that can guide their practice. But the reality is that epidemiology is limited; it is simply not as robust as we would like it to be in all situations. This means that sometimes health educators are making choices based on values, not science. Being clear about what those values are becomes crucial. When public health educators can articulate their values and balance market justice with social justice values, they will be able to transmit coherent, consistent, and compelling messages inside and outside the field.
Beauchamp's (1976) insights about public health as social justice have motivated a generation of health educators who have found themselves struggling against increasingly dominant market justice values. How the debate is framed, especially how it is framed in news stories, has had a profound effect on how Americans understand and relate to public problems. These analyses now can be used to reinforce and make tangible Beauchamp's notions of public health as social justice in the context of framing specific public health battles.
Lori Dorfman, Berkeley Media Studies Group, Public Health Institute. Lawrence Wallack, College of Urban and Public Affairs, Portland State University. Katie Woodruff, Berkeley Media Studies Group, Public Health Institute.
Address reprint requests to Lori Dorfman, Berkeley Media Studies Group, 2130 Shattuck Avenue, Suite 302, Berkeley, CA 94704; e-mail: dorfman@bmsg.org.
The authors thank Makani Themba-Nixon of the Praxis Project and George Lakoff and Pamela Morgan of the Rockridge Institute for their insights and innovative thinking about how to frame public policy battles. Dr. Wallack's work on this article was supported in part by an innovator's grant from The Robert Wood Johnson Foundation.
Health Education & Behavior, Vol. 32 (3): 320-336 (June 2005)
DOI: 10.1177/1090198105275046
© 2005 by SOPHE
References
Bagdikian, B. H. (2004). The new media monopoly. Boston: Beacon.
Barboza, D. (2003, July 10). A warning in expanding waistlines, food markets trim fast as lawsuits and new regulations loom. The New York Times, p. C1.
Beauchamp, D. E. (1976). Public health as social justice. Inquiry, 13 , 3-14.
Bellah, R., Madsen, R., Sullivan, W. M., Swidler, A., & Tiptom, S. M. (1985). Habits of the heart: Individualism and commitment in American life. Berkeley: University of California Press.
Bellows, J. (1998). Newspaper frames of childhood lead poisoning. Issue, 5.
Chapman, S. (2001). Advocacy in public health: Roles and challenges. International Journal of Epidemiology, 30, 1226-1232.
Chapman, S., & Lupton, D. (1994). The fight for pubic health: Principles and practices of media advocacy. London: British Medical Journal Publishing.
Chavez, V., & Dorfman, L. (1996). Youth and violence on local Spanish language television news. International Quarterly of Community Health Education, 7, 121-138.
Dorfman, L. (2003). Using media advocacy to influence policy. In R. J. Bensley & J. BrookinsFisher (Eds.), Community health education methods: A practitioner' s guide (2nd ed.). Sudbury, MA: Jones & Bartlett.
Dorfman, L., Ervice, J., & Woodruff, K. (2002, November). Voices for change: A taxonomy of public communications campaigns and their evaluation challenges. Paper prepared for the Communications Consortium Media Center, Media Evaluation Project, Washington, DC.
Dorfman, L., & Schiraldi, V. (2001). Off balance: Media coverage of youth crime. Guild Practitioner, 58, 75-78.
Dorfman, L., & Wallack, L. (1998). Alcohol in the news: The role for researchers. Contemporary Drug Problems, 25, 65-84.
Dorfman, L., Woodruff, K., Chavez, V., & Wallack, L. (1997). Youth and violence on local television news in California. American Journal of Public Health, 87, 1311-1316.
Entman, R. (1993). Framing: Toward clarification of a fractured paradigm. Journal of Communication, 43, 51-58.
Gamson, W. A. (1992). Talking politics. Cambridge, UK: Cambridge University Press.
Gilliam, F. D., Jr. (2003, December 19). Right for the wrong reasons. FrameWorks Institute Ezine, 26. Retrieved June 16, 2004, from http://www.frameworksinstitute.org/ezine26.html
Gitlin, T. (1980). The whole world is watching. Berkeley: University of California Press.
Harrington, M. (1999). Care and equality: Inventing a new family politics. New York: Routledge.
Iyengar, S. (1991). Is anyone responsible? How television frames political issues. Chicago: Chicago University Press. Jernigan, D., & Dorfman, L. (1996). Visualizing America's drug problems: An ethnographic content analysis of illegal drug stories on the nightly news. Contemporary Drug Problems, 23, 169196.
Lakoff, G. (1996). Moral politics: What conservatives know that liberals don't. Chicago: University of Chicago Press.
Lakoff, G., & Morgan, P. (2001). Framing social issues: Does "the working poor" work? (Report to the Ford Foundation; Rockridge Strategic Analysis Paper 2001-01). In Public obligations: Giving kids a chance (Report from a conference on the state role in early education, Innovations in American Government, Kennedy School of Government, Harvard University, pp. 16-38). Cambridge, MA: Harvard University Press.
Lawrence, R. (2002). American values and the news about children's health. Issue, 12.
Lippmann, W. (1922). Public opinion New York: Macmillan. McBride, S. (2003, November 15). Are soft drinks responsible for the obesity epidemic? Beverage World, p. 23.
McManus, J., & Dorfman, L. (2005). Functional truth or sexist distortion? Assessing a feminist critique of intimate violence reporting. Journalism, 6, 43-65.
National Public Radio. (2004, July 18). All things considered by Julie Rovner.
Novello, A. C. (1992). Underage drinking: A report from the surgeon general. Journal of the American Medical Association, 268, 961.
Pew Center Poll. (2002). What the world thinks in 2002, how global publics view: Their lives, their countries, the world, America. Retrieved October 26, 2004, from http://people-press.org/reports/display.php3?ReportID=165
Pynchon, T. (2000). Gravity's rainbow. New York: Penguin.
Reich, R. (Ed.). (1990). The power of public ideas. Cambridge, MA: Harvard University Press.
Smith, A. (2000). The wealth of nations. New York: Modern Library.
Themba, M. (1999). Making policy making change: How communities are taking the law into their own hands. Berkeley: Chardon.
Tronto, J. (1994). Moral boundaries: A political argument for an ethic of care. New York: Routledge.
Wallack, L., Dorfman, L., Jernigan, D., & Themba, M. (1993). Media advocacy and public health: Power for prevention. Newbury Park, CA: Sage.
Wallack, L., & Lawrence, R. (in press). Talking about public health: Developing America's second language. American Journal of Public Health.
Wallack, L., Woodruff, K., Dorfman, L., & Diaz, I. (1999). News for a change: An advocates' guide to working with the media. Thousand Oaks, CA: Sage.
Wintemute, G., Teret, S., Kraus, J., Wright, M., & Bradfield, G. (1987). When children shoot children: 88 unintended deaths in California. Journal of the American Medical Association, 257, 3107-3109.
Woodruff, K., Dorfman, L., Berends, V., & Agron, P. (2003). Coverage of childhood nutrition policies in California newspapers. Journal of Public Health Policy, 24, 150-158. Woodruff, K., & Villamin, E. (1997). Junk gun bans in California newspapers. Issue, 2.